Clinical Overview
Audience: clinicians & researchers • Updated
Abstract
This site summarizes the"SAER" benzodiazepine detox protocol authored by Anna Basińska‑Szafrańska, with emphasis on PK-awareness and the breakthrough (let's be humble here) role of lab feedback to safely and expeditiously guide the patient to adaptation to zero BZD serum concentration level
What does the SAER protocol promise?
- Concluding the true (details below) detoxification in (median) under 52 days
- 92% completion rate
- Comfortable patient's experience
- Low cost, as far as an inpatient treatment can be labeled "low cost"
What is the current status/record of the SAER protocol, as a medical procedure?
SAER protocol evolved in clinical practice of the detoxification unit in the Institute of Psychiatry and Neurology in Warsaw, Poland. Long story short, this allowed to raise the completion rate of BZD detox in the Institute from around 50% to 92%, with N approaching 1000.
At the moment (Fall 2025) the SAER protocol is documented in https://doi.org/10.1159/000547221. A series of papers analyzing the underlying issues in detail has been published over last 10 years. The protocol itelf is ready to be verified in clinical practice outside the Institute of Psychiatry and Neurology. We would welcome practitioners and researchers interested in more information and/or training and collaboration.
What novel elements are involved in the SAER protocol?
The main issue is PK-awareness. It has to be stressed that the SAER protocol uses exclusively the clinical and lab criteria, not modeling/calculations. But to understand the rationale of the protocol, being aware, qualititavely, of the underlying pharmacokinetic issues is essential.
The single most important element is realization that a "succesfull BZD detox" means "adaptation to zero concentration of active benzodiazepines in patient's blood serum". This is VERY different from "adaptation to BZD abstinence", as some BZDs have very long elimination half-times. Moreover, the elimination process individually varies in the extreme, due to patient's age, some BZDs affinity to adipose tissues and many other factors.
Consequently, what was commonly called "patient's adaptation to a given dose" (or to a null dose, meaning absitinence), was actually adaptation to patient's current serum BZD concentration, of which, without a direct measurement, not much can be inferred (below). While the dose can be kept steady, serum concentration cannot, without a lab feedback.
Until now, the consensus among practitioners and researchers was that BZD serum measurements throughout the detox treatment is pointless. This position was thought to be justified by complex pharmacokinetics of commonly used BZDs and individual variations, both of PK and PD. So the consensus emerged that BZD detox should be driven only by patient's feedback and overly cautious schedules. Serum measurments could be used, the thinking went, if at all, only to test for compliance.
Unfortunately, this "makes no practical sense to think about PK too much" paradigm has led to common and unrecognized serious procedural errors, harming the patients.
What errors in the common detox protocols does the SAER protocol address?
- Concluding the detox after several days of patient's BZD abstinence. Patients are told "you are now free of BZD dependence" and discharged, while they are still high on residual BZDs. This results in a withdrawal crisis, often leading to relapse.
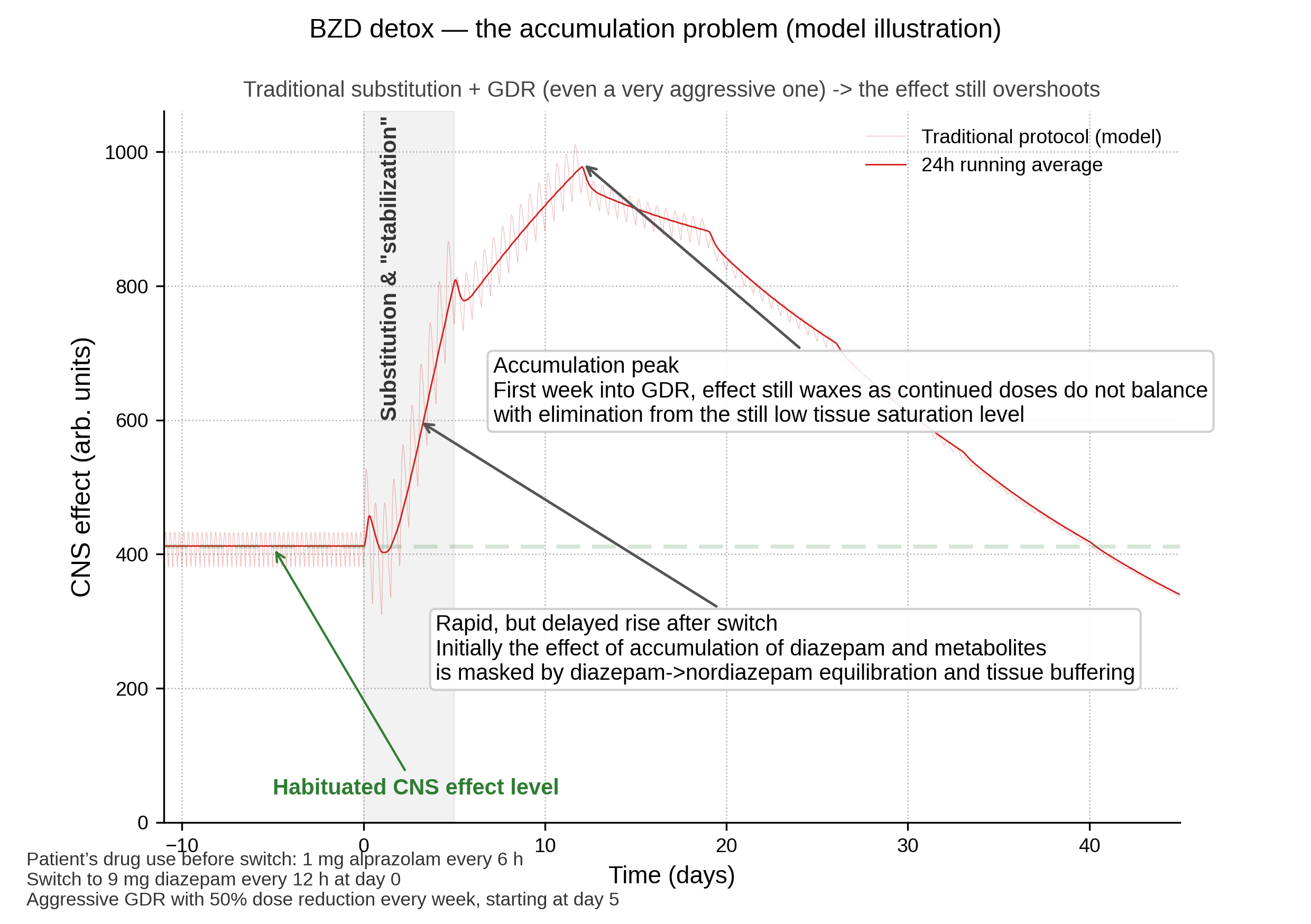
- Intoxicating the patients during the "long acting BZD substitution" stage, due to drug accumulation. While purposeful measurement would be unethical, it was exactly this phenomenon, measured serendipously, which gave a push into the research resulting in SAER development.
- Unnecessary long detoxification (details in the bibliography)
What new tools made SAER practical?
When the now (2020s) used detox protocols were developed, there were no tools available to monitor serum BZD concentration, as far as practical clinical application was concerned. Hence the protocols were "conservative", to accomodate the most extreme variations between individuals, variations which could not be measured in clinical practice. Clinicians did, back then, the best they could.
Today the immunoassays can ROUGHLY quantify BZD serum levels with accuracy and detection thresholds which make SAER possible. Those assays "could be better", but they will do. And they are vastly cheaper than the precise methods. The added cost of using immunoassays is miniscule.
Disclaimer. This material is informational and does not substitute individualized clinical judgment. Always consider local regulations and patient‑specific factors.